Latest Research & News
Insights and findings from our medical research community.
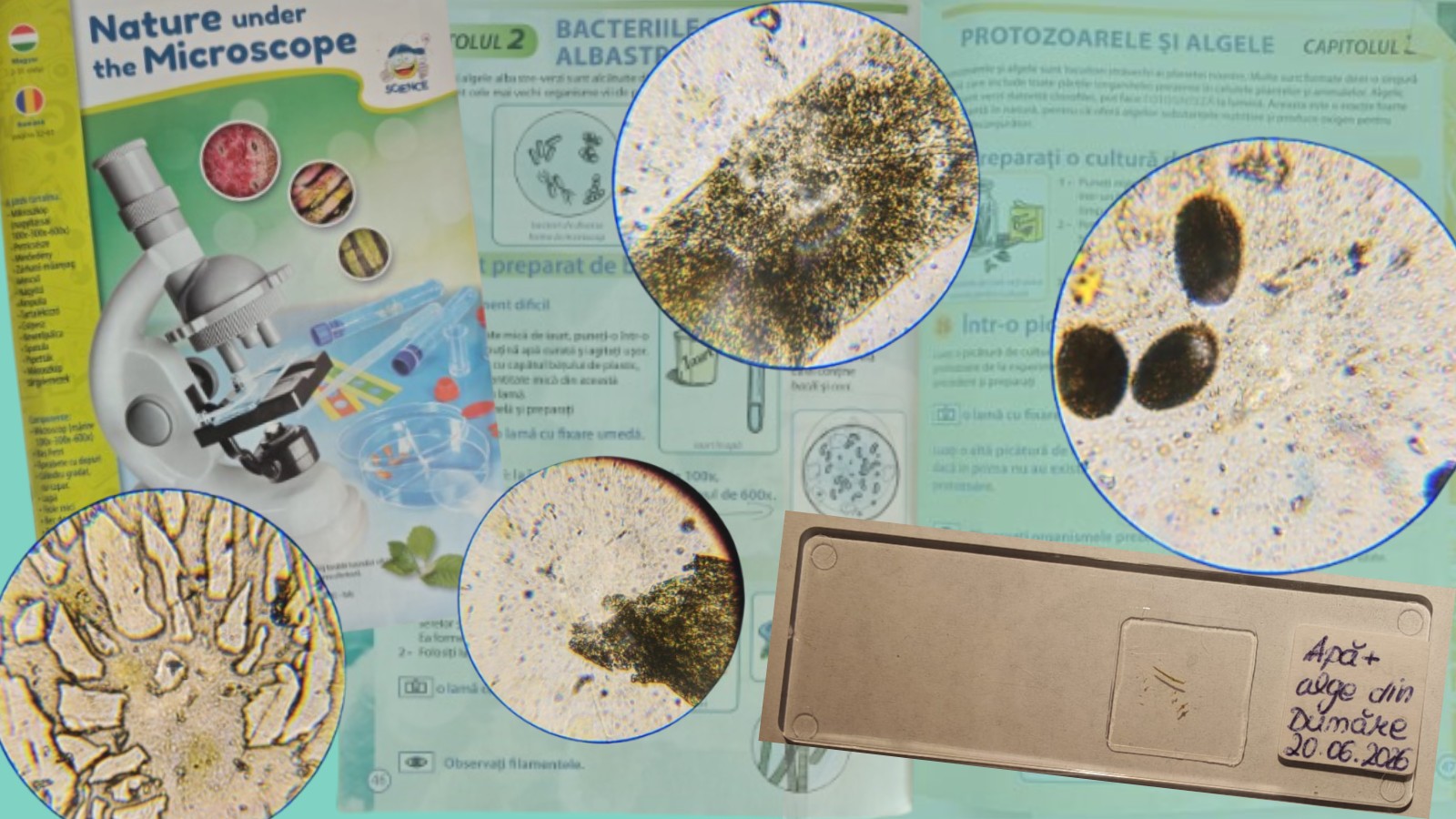
Microscopic study of river water and pollen germinationThis week, I continued exploring one of my hobbies: microscopy. Interested in the natural world, I kept experimenting with observations under the microscope using a guide I have been following. In particular, I wanted to revisit Experiment 38, which focuses on pollen germination, as I was curious whether I could obtain different or clearer results compared to my previous attempt.While going through the guide, I also came across an experiment I had always wanted to try: observing green algae under the microscope and possibly studying them in a simple home setup without laboratory equipment. For this purpose, I collected a water sample during a boat trip on the Danube, which also contained visible traces of algae floating in the water.I am aware that the Danube area includes protected ecosystems, especially for species such as yellow and white water lilies, which are endangered. For this reason, I made sure to collect only water from open areas, avoiding any disturbance of aquatic plants or surrounding habitats.After one week, I examined the sample. Upon opening the test tube containing the river water and algae, I noticed a very strong, pungent and unpleasant odor, likely caused by natural decomposition processes. To safely handle the sample, I used gloves and two protective face masks during the experiment.Microscopic observation of river water and algaeFirst, I placed a drop of river water onto a microscope slide using the wet mount technique. Simply put, a wet mount is a microscopy method for observing liquid samples using a cover slip to improve clarity under the microscope.I also isolated a small portion of the algae sample, as it appeared to have small particles attached to its surface, possibly sediment or microorganisms from the river environment.I took photos at each magnification level (100×, 600×, and 1200×) using my phone.At lower magnification, a green filamentous structure was visible, which I identified as the algae sample. Around it, there were small particles and sediment from the riverbed, which is expected in natural water samples. At higher magnification, a transparent structure became more visible, containing small yellowish dots arranged in a pattern that resembled a chain or ladder-like structure. While I cannot precisely identify its nature, it appeared to be part of the algae’s internal or attached structure and was particularly interesting to observe.I had also hoped to observe more diverse or “ancient” forms of algae, similar to those found in more isolated environments, but the sample mainly reflected a typical river ecosystem. Nevertheless, it provided valuable microscopic detail.Pollen germination experimentThe second part of the experiment focused on pollen germination. Following the instructions in the guide, I prepared a sugar solution by dissolving sugar in water. I then collected pollen from lilies, plants known for their strong fragrance and highly visible pollen grains, and mixed it into the solution. The sample was left to sit for approximately three hours.After this period, I placed a drop of the solution onto a wet mount slide. The solution had taken on an orange tint due to the pollen pigments.Under the microscope, I observed multiple brown oval structures, which I identified as pollen grains. At higher magnification, smaller yellow particles were visible around some of the pollen grains. Based on their appearance, these may correspond to pollen germination structures, although this remains a qualitative observation.Previous attempt and comparisonI had performed a similar experiment approximately two years ago. However, due to an issue with the wet mount preparation, the cover slip detached, and I attempted to fix it using super glue. This likely altered the chemical composition of the sample, especially the sugar solution and pollen interaction, resulting in different visual outcomes compared to the present experiment.ConclusionOverall, these experiments provided a valuable opportunity to practice basic microscopy techniques and explore my interest in the microscopic world. Each attempt gives me a better understanding of what can be observed under the microscope and keeps my curiosity going.References->Microscopy guide used for educational purposes->Personal observations and experiments
New research is revealing how our immune cells "remember" experiences, opening the door to more personalized treatments for chronic diseases.Our immune system is far more adaptable than scientists once believed. While our DNA provides the blueprint for how our bodies function, another layer of regulation—known as epigenetics—determines how that blueprint is used.Recent research has shown that epigenetic changes play a key role in controlling macrophages, one of the body's most important immune cells. Understanding how these cells adapt could transform the way we prevent and treat inflammatory, autoimmune, and neurodegenerative diseases.What Are Macrophages?Macrophages are specialized immune cells that protect the body by: Detecting and eliminating harmful bacteria and viruses Removing damaged or dead cells Supporting tissue repair and healing Coordinating the body's inflammatory responseRather than behaving the same way throughout the body, macrophages adapt to the environment around them. Those found in the lungs, liver, skin, or brain each perform unique functions tailored to the needs of that tissue.What Is Epigenetics?Although nearly every cell in the body contains the same DNA, not every gene is active at the same time.Epigenetics refers to the biological mechanisms that switch genes on or off without changing the DNA sequence itself. These changes help cells respond to their environment, allowing the immune system to react quickly to infections, injuries, and other challenges.One of the most important epigenetic mechanisms involves chromatin—the structure that packages DNA inside our cells. When chromatin becomes more open, certain genes become easier to activate, enabling macrophages to rapidly adjust their behavior when needed.The Immune System Can "Remember"Scientists have recently discovered that macrophages can develop a form of trained immunity.Unlike the long-term memory created by antibodies, trained immunity is driven by epigenetic changes. After exposure to infections or inflammation, macrophages can become "primed" to respond more effectively—or, in some cases, too aggressively—to future challenges.This growing field of research may help explain why chronic inflammation contributes to conditions such as: Cardiovascular disease Type 2 diabetes Autoimmune disorders Alzheimer's disease Parkinson's diseaseWhy This MattersThe brain contains its own specialized macrophages, called microglia, which help protect neurons and maintain healthy brain function.When these cells remain activated for long periods, they can contribute to ongoing inflammation that has been linked to several neurodegenerative diseases. By understanding the epigenetic signals that control these immune cells, researchers hope to develop therapies that regulate inflammation without suppressing the immune system entirely.Looking AheadAdvances in genomics and epigenetics are changing our understanding of the immune system. Rather than viewing immune cells as fixed responders, scientists now recognize that they are highly adaptable and continuously shaped by their environment.As research continues, these discoveries may lead to more precise treatments that target the underlying mechanisms of disease instead of simply managing symptoms. This represents an important step toward the future of precision medicine, where therapies can be tailored to each individual's unique biological profile.
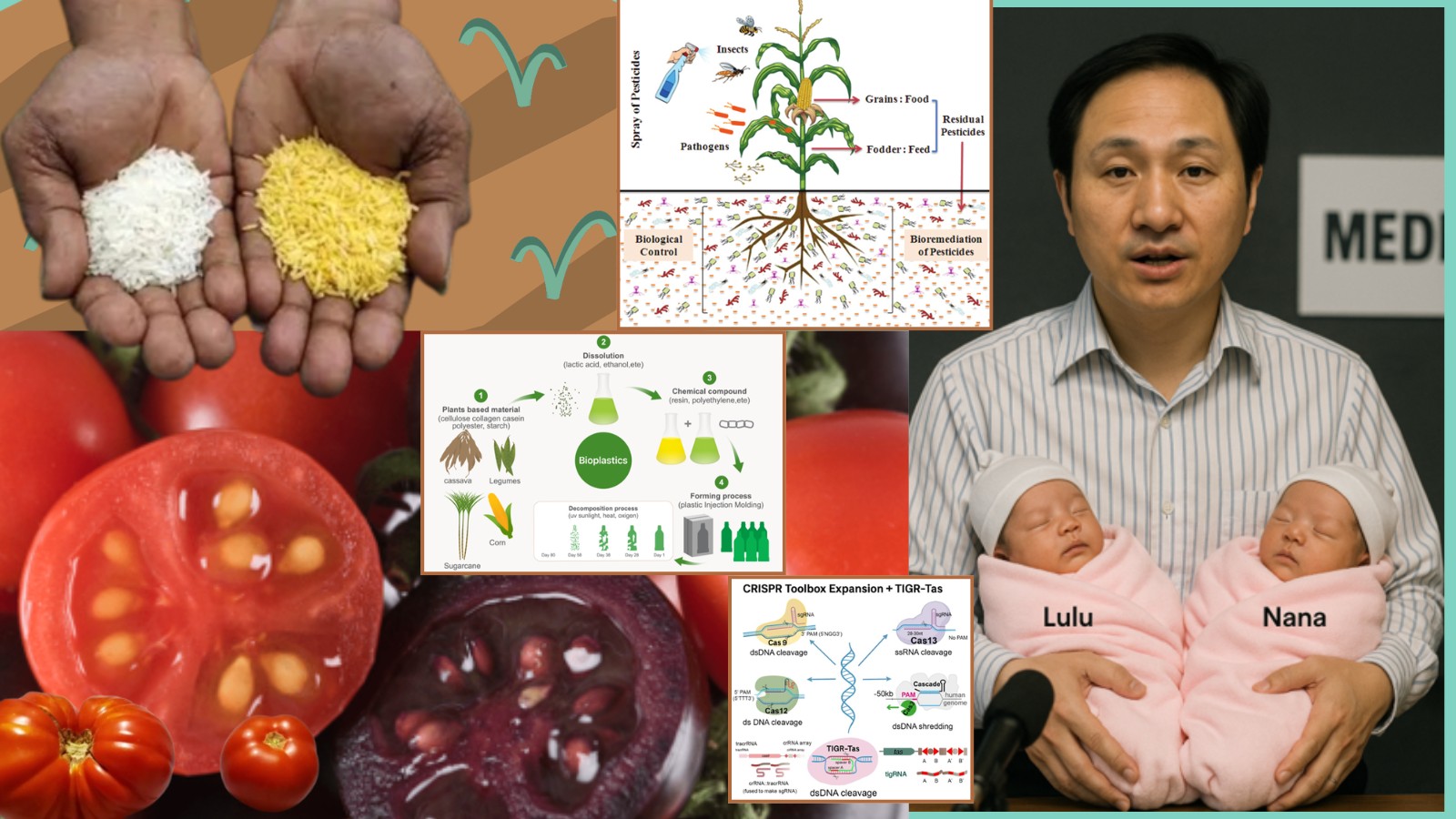
Genetic EngineeringPS: This article was developed as part of a school biology project. It is the result of collaborative work, including shared research, documentation, and organization of the material. The aim of the project was to explore key concepts in modern biology, with a particular focus on genetic engineering, and to present the information in a clear and structured academic form.Introduction to Genetic EngineeringGenetic engineering is a branch of biology focused on the modification of an organism’s genetic material (DNA). Its purpose is to introduce, remove, or modify specific genes in order to obtain desired traits, such as resistance to diseases or the production of useful substances like medicines.This field emerged from the need to better understand and control biological processes. The first experiments began in the second half of the 20th century, alongside the development of recombinated DNA technology.How Genetic Engineering WorksThe process of genetic engineering involves several key steps:-identifying a gene with a useful function-isolating or copying that gene from an organism-inserting the gene into the DNA of another organism-multiplying or reproducing the modified organismA very important technology in this field is CRISPR-Cas9, often described as “molecular scissors” that can cut DNA at precise locations. This technology has made genetic modification faster, cheaper, and far more accurate than previous methods.CRISPR-Cas9CRISPR-Cas9 (Clustered Regularly Interspaced Short Palindromic Repeats – Cas9 protein) is one of the most important discoveries in modern biology. It allows scientists to edit DNA with high precision, similar to editing text on a computer.Bacteria naturally use this system as a defense mechanism against viruses. They store fragments of viral DNA in their genome within CRISPR regions. When the virus attacks again, the bacterium:>recognizes the viral DNA>produces a guide RNA>directs the Cas9 protein to the matching sequence>cuts and destroys the viral DNAScientists Jennifer Doudna (UC Berkeley) and Emmanuelle Charpentier (Max Planck Institute) demonstrated that this mechanism can be adapted for gene editing in plants, animals, and humans.TIGR-Tas TechnologyTIGR-Tas is a newly developed gene-editing system (2025) created by researchers at the Massachusetts Institute of Technology and the Broad Institute. It uses RNA-guided proteins to target specific DNA sequences, similarly to CRISPR-Cas9.Its main advantages include:--smaller protein size compared to Cas9, making delivery into cells easier--the use of two guide RNA sequences, potentially increasing precision--no requirement for a PAM sequence, allowing access to more genomic targetsResearchers consider TIGR-Tas a promising future tool for gene therapy and biomedical research.Ethical Considerations in Genetic EngineeringGenetic engineering offers major benefits but also raises ethical concerns. On one hand, it can treat genetic diseases and improve agriculture through more resistant crops. On the other hand, it raises concerns about altering natural systems and unknown long-term effects on ecosystems and organisms.A particularly controversial issue is human genetic modification, which could lead to inequality, misuse of technology, and ethical conflicts. For this reason, bioethics emphasizes that genetic engineering must be used responsibly and strictly regulated.Applications of Genetic EngineeringMedical ApplicationsGenetic engineering has transformed modern medicine by enabling innovative therapies and advanced diagnostic techniques.Examples include:-production of insulin using genetically modified bacteria, reducing allergic reactions and replacing animal sources-gene therapy for correcting defective genes in inherited diseases such as cystic fibrosis-development of modern vaccines, including those for COVID-19, hepatitis B, and HPV-modification of immune cells to improve cancer treatmentAgricultural ApplicationsGenetic engineering has led to the development of crops with improved characteristics that address global challenges. These plants may be resistant to pests, reducing pesticide use, or tolerant to herbicides, improving weed control.Examples include:--Golden Rice, enriched with vitamin A precursors to combat nutritional deficiencies--genetically modified tomatoes with longer shelf life, reducing food waste--purple tomatoes rich in anthocyanins with added health benefits--drought- and salt-resistant crops adapted to climate change--plants engineered to fix nitrogen, reducing the need for chemical fertilizersIndustrial ApplicationsGenetic engineering is widely used in industry to produce useful substances through genetically modified microorganisms acting as bioreactors.Examples include:--enzymes used in detergents, textiles, and food processing--biofuels such as ethanol and biodiesel produced from biomass--biodegradable plastics and biomaterials as alternatives to petroleum-based productsEnvironmental ApplicationsGenetic engineering provides solutions for pollution reduction and ecosystem protection.Examples include:--microorganisms used in bioremediation to break down oil, pesticides, and heavy metals--biological biosensors for detecting toxic substances in the environment--bacteria used to clean oil spills in oceans--conservation efforts for endangered species and biodiversity protectionResearch ApplicationsGenetic engineering helps scientists study biological processes using genetically modified organisms as research models.Examples include:--animals and plants used to study human diseases and test treatments--genetically modified mosquitoes to reduce malaria transmission--gene-editing tools used to understand gene function--synthetic biology for designing new biological systemsAdvantages of Genetic Engineering--more effective and safer medical treatments--increased agricultural productivity--reduced pesticide use and environmental pollution--environmental protection through bioremediation--production of sustainable medicines and materialsDisadvantages of Genetic Engineering--unknown long-term risks--potential negative effects on ecosystems--uncontrolled spread of modified genes--high costs of technology--ethical concerns regarding human genetic modificationsEthical Controversy: The He Jiankui CaseIn 2018, Chinese researcher He Jiankui announced that he had used CRISPR-Cas9 gene-editing technology to modify human embryos with the aim of making them resistant to HIV infection. He targeted the CCR5 gene, which plays a role in allowing HIV to enter human cells. According to his claims, the edited embryos were implanted and resulted in the birth of twin girls.The experiment quickly sparked global controversy because it was carried out without clear, internationally recognized ethical approval and with limited transparency. Questions were raised about whether the parents gave fully informed consent and whether the research followed proper regulatory procedures.Scientists around the world strongly criticized the work. Many argued that it was unnecessary, since HIV can already be effectively prevented through existing medical methods, and that editing embryos introduced serious risks. One major concern was the possibility of off-target genetic changes, as well as unknown long-term effects that could affect not only the children but also their future descendants, since germline edits are heritable.Following the announcement, the case led to widespread condemnation, legal consequences for He Jiankui in China, and renewed global debate about how and when human embryo editing should be allowed. It is now widely seen as a landmark example of unethical application of genetic engineering and a warning about the need for stronger international oversight.ConclusionGenetic engineering is a major scientific field with applications in medicine, agriculture, industry, and environmental protection. It offers significant progress in treating diseases, improving food production, and reducing pollution, but also raises ethical challenges and risks that require responsibility and strict regulation.Future technologies such as CRISPR-Cas9 and emerging systems like TIGR-Tas may enable even more precise and effective solutions for health and the environment, provided they are used ethically and under proper control.Bibliography / SourcesMed.Ro – Genetic engineering: applications, benefits and risksȘtiința Azi – What is genetic engineering (CRISPR)Revista Română de Bioetică – What is genetic engineering? A fundamental introductionAmerican Association for the Advancement of Science (AAAS) – Chinese scientist who produced genetically altered babies sentenced to 3 years in jailMIT Technology Review – A controversial Chinese CRISPR scientist is still hopeful about embryo gene-editing. Here’s whyCenters for Disease Control and Prevention (CDC) – Genetically Modified MosquitoesScience (AAAS) – https://www.science.org/doi/10.1126/science.adv9789PubMed Central (PMC) – https://pmc.ncbi.nlm.nih.gov/articles/PMC9377665/Image sources:https://3.bp.blogspot.com/-3DMovUHqoYU/UbnMpwYUNvI/AAAAAAAABOI/OrUicRTNMpA/s1600/stem+cell.JPG+190.JPGhttps://blogger.googleusercontent.com/img/b/R29vZ2xl/AVvXsEhQxXyy3b8iuOsneSg11rAsl16v6_5gXCZDTkte6W5oaTM_vgxB3v6lbyYxsB47OfczddcgXjlJB3hLqdl615-gj2Bjx9pUQ9gzXTZmwIF2aTSQrYbaXKxxsd5LzLVEqnV6YzgTGhnTnec-fzcb7viv-p-nJIrUpLGddK-UM8S1MwTbLQbCi82uygIzyCE/s1536/file_0000000038e061f9b3e797598e0903f4.pnghttps://www.researchgate.net/publication/349706113/figure/fig2/AS:996785300439046@1614663543638/Applications-of-genetic-engineering-and-genome-editing-to-improve-plant-molecular-farming_Q640.jpghttps://scx2.b-cdn.net/gfx/news/hires/2020/3-engineeringa.jpghttps://media.licdn.com/dms/image/v2/D5612AQGjWpnmvuBg3A/article-cover_image-shrink_600_2000/article-cover_image-shrink_600_2000/0/1697795146425?e=2147483647&v=beta&t=CTNFpShKYFwLXSuFVwfhaOoUPcdTU6nFGtqcf7ajukUhttps://cdn.ncbi.nlm.nih.gov/pmc/blobs/3f0e/4914850/2e9ce91d1645/srep27185-f1.jpg
If you're one of the more than 170 million women worldwide that have been told they have PCOS (Polycystic Ovary Syndrome), you might be interested in what I'm about to tell you!On the 12th of May 2026, The Lancet published a massive global consensus. After over a decade of advocacy, research, and pushing by patients and doctors, the name PCOS is officially being retired.Say hello to PMOS: Polyendocrine Metabolic Ovarian Syndrome.This isn't just medical jargon or a boring textbook update. It is a massive, historic victory for how women’s bodies are understood and treated. Here is why this name change is going to change lives.The Biggest Misconception : There are No Cysts!Let's start with the most frustrating part of the old name. For decades, the word "polycystic" made people think they had dangerous, exploding cysts on their ovaries. But biologically, that's completely wrong. The "cysts" seen on ultrasounds are actually just antral follicles; perfectly normal, tiny fluid-filled sacs that contain immature eggs. Because of hormonal imbalances, the body just gets confused, and ovulation gets paused. The eggs get stuck in their early development stages, leading to a high volume of these follicles (20 or more).Calling it an ovarian cyst disease did two really damaging things:1. It made people think it was just a "reproductive issue" you only need to worry about when you want to get pregnant.2. It completely ignored everything else happening in the rest of the body, leading to missed diagnoses, given treatment you might not even need, and years of frustration.Breaking Down PMOS: Why the New Name Actually Makes SenseThe new name, PMOS, finally looks at the whole picture. It’s broken down into three pillars that perfectly describe what’s actually going on:1. Polyendocrine (The Hormone Chaos)"Poly" means many, and "endocrine" refers to your hormones. This acknowledges that the condition isn't just about estrogen or progesterone. It’s a complex web involving high androgens (like testosterone) and messed-up signaling between the brain and the ovaries.2. Metabolic (The Missing Piece)This is the absolute most important change. Including "metabolic" finally forces the medical world to recognize that this condition is deeply tied to insulin resistance. This isn't just about irregular periods; it carries lifelong risks for:- Type 2 diabetes- Cardiovascular issues and high blood pressure- Metabolic syndrome3. Ovarian (The Effect, Not the Cause)The ovaries are still in the name because, yes, irregular cycles and fertility struggles are a major part of the experience. But now, the ovaries are recognized as being affected by the systemic hormone and metabolic issues, rather than being the root cause of the entire problem.What Actually Causes PMOS?If you have it, it is not your fault. Here is what is actually going on under the hood:- Insulin Resistance: This is the big one. Your cells stop responding properly to insulin, so your pancreas pumps out way too much of it to compensate. Here is the kicker: high levels of insulin actively signal your ovaries to produce too much testosterone.- Low-Grade Inflammation: People with PMOS often have chronic, low-grade inflammation. This stimulates polycystic ovaries to produce androgens, which further drives the metabolic cycle.- Genetics: If your mom, sister, or aunt has PMOS (or Type 2 diabetes), your chances of having it are much higher. Certain genes are heavily linked to how your body processes hormones and insulin.- Androgen Excess: The ovaries produce abnormally high levels of male hormones (androgens), which throws off the delicate feedback loop between your brain's pituitary gland and your reproductive system, stopping normal ovulation.The Reality Check: Serious Long-Term ComplicationsThis is exactly why the name change to include "Metabolic" is so critical. PMOS isn't just about acne, facial hair growth (hirsutism), or irregular periods. If left unmanaged, the chronic hormonal and metabolic chaos can lead to serious, life-altering complications:- Type 2 Diabetes & Pre-diabetes: Because of chronic insulin resistance, more than half of women with PMOS develop type 2 diabetes before the age of 40.- Cardiovascular Disease: High insulin and inflammation lead to high blood pressure, elevated LDL ("bad") cholesterol, and clogged arteries, significantly increasing the risk of heart attacks and strokes later in life.- Infertility: Because ovulation is irregular or entirely absent (anovulation), PMOS is the leading cause of female infertility worldwide.- Pregnancy Complications: When patients with PMOS do get pregnant, they face much higher rates of gestational diabetes, preeclampsia (dangerously high blood pressure), and premature birth.- Endometrial Cancer: If you don't menstruate regularly, the lining of your uterus (the endometrium) builds up month after month without shedding. This continuous exposure to estrogen without enough progesterone increases the risk of uterine cancer.- Non-Alcoholic Fatty Liver Disease (NAFLD): Severe insulin resistance causes fat to accumulate in the liver, which can lead to chronic liver inflammation and scarring.- Mental Health Struggles: The physical symptoms, weight struggles, and hormonal imbalances create a massive toll on mental health. People with PMOS are statistically at a much higher risk for clinical depression, severe anxiety, and eating disorders.How will this affect the future of care?Well first and foremost, the standard infrastructure for this procedure will change:- Where the doctor did a pelvic ultrasound for PCOS, they will now look at your bloodwork, metabolic health, and your symptoms as a whole (!)- Secondly, they can't just prescribe you a birth control and hoping for the best. Instead, they will need to have a whole team of endocrinologists, dietitians and so on who focus on your wellness as a whole.- Furthermore, being dismissed because your ovaries look "just fine" can't happen anymore, they will need to take your symptoms and hormonal disruptivenesses in complete consideration.Because the core diagnostic criteria is remaining how they were, and the recent changes having been made, there is a three-year transition plan in place to officially weave PMOS into healthcare systems worldwide by 2028, to fully ensure that medical coding systems and global guidelines are being updated.A Personal Note - Why this is so Important to meFor way too long, women's health has been sidelined, underfunded, and misunderstood. Patients have had to become their own researchers just to get basic answers.Changing the name to PMOS strips away a century of medical misconception. It forces the healthcare system to look at young women not just as reproductive vessels, but as whole people who deserve comprehensive, metabolic, and preventative care. We are finally being seen, and as a future provider, I could not be more proud or excited for where medicine is heading!
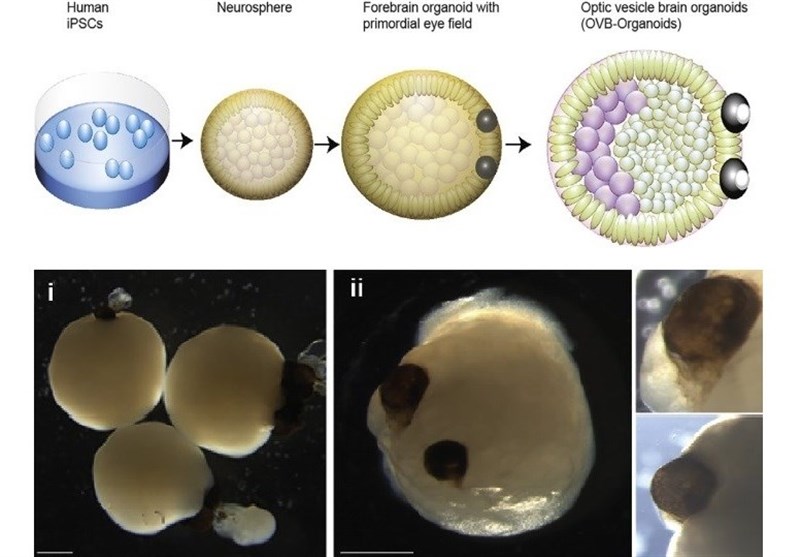
A few days ago I came across a post from Linkedln from Tuqa Mahdi taking about scientists growing "tiny brains in laboratories". At first it sounded like something pulled straight out of a sci-fi movie, but the more I looked in to it the more I realized its not really science fiction, at least not anymore.SO WHAT EXACTLY DID SCIENTISTS GROW?When people hear the phrase "scientists grew a brain" they often imagine a full and functioning brain floating into a glass container but that's not quite what exits today. Researchers instead grow something called a brain organoidThis brain organs is a tiny simplified model of brain tissue created from human stem cells. Stem cells are special because they can transform into many different type of cells inside the body. Scientists can guide these stem cells into becoming neurons and other brain related cells. Over time these cells begin organizing themselves into three-dimensional structures that resemble parts of a developing human brain. Most of the organoids are extremely small-often only a few centimeters wide many of these resemble a brain of a really stage fetal brain development rather than one of an adult. Even if they are tiny they can still do quite remarkable things: Mimic certain aspects of learning and memory, Form neuron activities, React to simulation.SO WHY EXACTLY ARE SCIENTISTS GROWING THESE BRAIN ORGANOIDS?The human brain is one of the most complex structures in existence. For decades neuroscientists struggled with a problem that it is extremely difficult to study living human brain tissue directly. Animal testing can only reveal part of the picture because human brains work differently from mouse or rat brains in many important ways.Brain organoids give researchers a new tool.Instead of experimenting on living people, scientists can observe miniature brain-like systems in controlled laboratory conditions. This can open the door to studying a lot of things such as: Alzheimer's disease, Parkinson's disease, Autism spectrum disorders, Epilepsy, Schizophrenia, Drug responses.Researchers can even grow organoids using cells from individual patients. That means future treatments could potentially become highly personalized.Imagine testing medication on a miniature version of a patient’s own neural tissue before prescribing it.THE BREAKTHROUGH THAT STARTED GETTING ATTENTION ONLINEIn recent years, several experiments pushed brain organoids into mainstream conversations.One of the biggest reasons people started posting about this topic online was because researchers discovered that some organoids were displaying surprisingly advanced neural behaviors. Scientist discovers thing such as: Rhythmic electrical signals similar to early human brain development, Early signs of adaptive learning, Basic memory related process. Researchers at Johns Hopkins recently reported evidence suggesting that certain organoids demonstrated the “building blocks” required for learning and memory. Another major development came from experiments where scientists connected organoids to computer systems through electrodes.These systems allowed the organoids to receive information and respond to stimuli. Some experiments even trained organoid systems to perform very basic computational tasks.That is where the phrase “organoid intelligence” started appearing.And yes — that phrase sounds like it belongs in a cyberpunk novel.ORGANOID INTELLIGENCE: BIOLOGY MEATS COMPUTINGOne of the most futuristic aspect in this field is the idea that biological neurons could eventually complement traditional computer chips. Today’s artificial intelligence systems run on silicon hardware. But biological brains are incredibly energy-efficient compared to modern computers. The human brain consumes roughly as much energy as a light bulb while outperforming even the most advanced AI systems in areas like adaptability, pattern recognition, and general learning. So we raise the question: What if scientists could harness living neural tissue for computing? Some companies and research labs are already exploring this possibility. Researchers have connected brain organoids to electrodes and digital systems to study how they process information.In some experiments, organoids learned to respond more effectively to repeated stimulation over time. One study even involved organoid systems improving performance on a simplified engineering task after receiving feedback.This does not mean scientists created conscious AI. However, it does suggest that living neural tissue may possess useful adaptive properties for future computing systems.NOW COULD SCIENTISTS EVER GROW A FULL HUMAN BRAIN?This is probably the question most people immediately ask. Technically speaking, modern science is nowhere near creating a complete conscious human brain in a lab.There are enormous limitations such as the fact that a living brain depends on: blood vessels, hormonal system, sensory imput, body interactions, immune system. Current organoids remain highly simplified. One major issue is that organoids often struggle to survive long-term because they lack full vascular systems capable of delivering oxygen and nutrients efficiently. Researchers are actively working on solving these problems. Some recent studies experimented with creating blood vessel-like structures inside organoids. Even so, scientists remain extremely far from building a complete human brain.AND SOME OF MY FINAL THOUGHTSThat LinkedIn post I saw initially sounded like clickbait. But after researching the topic more deeply, I realized the reality is actually more interesting than the headlines. Scientists are not secretly building fully conscious brains in underground laboratories. What they are doing is creating tiny brain-like systems that could revolutionize medicine, neuroscience, and computing. At the same time, these breakthroughs force humanity to confront questions we have never truly faced before.If biology can eventually merge with computation…If living neural systems can process information…If miniature brain tissue can learn and adapt…Then the boundaries between technology and life may become increasingly difficult to define. Whether this field ultimately becomes one of humanity’s greatest medical achievements or one of its most controversial scientific frontiers will depend not only on the technology itself, but on the ethical decisions society makes along the way.And honestly, that may be the most important part of the entire conversation.
We are called the prestatiegeneratie. VWO and Gymnasium students are expected to excel in eight subjects, build an impressive extracurricular resume, and maintain a flawless social life, all while deciding their entire academic future by age 17. The Netherlands historically prided itself on a relaxed "zesjescultuur" (a six-is-good-enough culture). But that era is dead. Today, research from the Trimbos-instituut reveals that approximately 1 in 3 Dutch youths suffer from severe performance pressure (Dopmeijer, n.d.). The pressure isn't just psychological. It is deeply, structurally biological. When academic stress becomes chronic, it actively alters the developing teenage brain.The HPA-Axis and the Exam HallWhen a student stares at a crucial final exam, the brain does not differentiate between the threat of a failing grade and the threat of a physical predator. The physiological alarm sounds.This alarm system is the Hypothalamic-Pituitary-Adrenal (HPA) axis. The hypothalamus secretes Corticotropin-Releasing Hormone (CRH), which signals the pituitary gland to release ACTH into the bloodstream. This eventually commands the adrenal glands to pump out the primary stress hormone: cortisol (Romeo, 2013). In short bursts, cortisol is a lifesaver. It sharpens focus, mobilizes glucose for energy, and helps you power through a difficult test.The problem with the prestatiegeneratie is that the stress never stops. Academic pressure is not a lion that chases you for ten minutes and then leaves. It is a constant, low-level hum of anxiety extending over years. This chronic activation breaks the HPA axis's negative feedback loop. The brain essentially forgets how to turn the alarm off.A Brain Under ConstructionThis chronic exposure to cortisol would be damaging to an adult, but for a Gymnasium student, it is uniquely toxic. The adolescent brain is highly plastic and still under heavy construction.During puberty, the brain develops back-to-front. The amygdala—the brain’s emotional processing and fear center—matures rapidly. However, the prefrontal cortex (PFC), which is responsible for rational decision-making, planning, and regulating those intense emotions, takes much longer to develop (Tottenham & Galván, 2016). The PFC is the part of the brain that is supposed to say, "Relax, it is just one math test, your life isn't over." But because the teenage PFC is still immature, the hyper-active amygdala takes the wheel.Furthermore, the developing adolescent brain is packed with a much higher density of stress hormone receptors than an adult brain (Tottenham & Galván, 2016). When you flood this highly sensitive, still-developing system with chronic cortisol for six years of high school, the neurobiological consequences are severe. Prolonged cortisol exposure actually shrinks the dendrites in the hippocampus (the brain's memory center), making learning harder—the exact opposite of what a stressed student needs. It also impairs the development of the PFC while reinforcing the neural pathways of fear and anxiety in the amygdala.We are not just burning out our youth psychologically. We are fundamentally rewiring their neurobiology for a lifetime of chronic stress.
In the medical world, nothing can really be compared to mental issues and psychological disorders, and this is sooner or later discovered by pretty much anyone who has got to understand medicine, even in its slightest. It is widely known that diseases which affect other parts of the body are most of the time curable or at least possible to be identified thanks to the patient’s sanity and collaboration with the medical experts – that, however, is not the case for many of the issues that target the brain. As the main organ in our body, essentially the pinnacle of the human power and identity, damaging it often brings horrific outcomes – the loss of one’s capacity to think or communicate, losing the sense of awareness and presence are many of the various well-known symptoms that shaped psychiatry into being probably one of the most disturbing medical fields to work in.This list, however, has another intention, and that is not to present the regular, common diseases that both doctors and medical professionals already have extensive experience with, such as schizophrenia or bipolar disorder – quite frankly, our today’s topic features the more peculiar, obscure and utterly horrific cases that haunted the medical field for quite some time – and for a good reason, as these are, as the title suggests, the rarest medical syndromes in the world. 1. Alice in Wonderland syndrome In order to properly understand why this syndrome got its funny name, we first must have a slight understanding of the novel’s topic: Alice in Wonderland explores the tale of a young girl that travels through a magical land, where time and space are distorted – therefore the effects are understandable – victims of this condition feature visual and reality distortions, which result in more than 60 different phenomena, from which we are going to mention the most important:- People and objects appear smaller (which is known as micropsia), and also the opposite way, with elements seeming bigger than in reality (this is called macropsia);- Other elements, including faces or whole bodies looking distorted (a phenomenon known as metamorphopsia);- Objects appearing closer than their actual distance is (this is named pelopsia), and the opposite effect, of objects looking farther than in reality (medically called teleopsia);- Hallucinating marked by seeing the same element or face many times (known as polyopia).Outside the visual distortions we mentioned above, patients also suffer from an altered perception of time and the feeling they are or detached from their own body and feelings (which is called depersonalization) or that they are disconnected from the external world (this is named derealization). All these symptoms appear in episodes that last about 30 minutes on average.The disturbing part of this condition is that an accurate incidence rate is currently unknown, which is especially because of the extremely low sickness rate – only about 150 cases in recorded medical history.The causing factors of this condition vary between multiple sources that specialists managed to identify. People at risk of this syndrome included those who already suffer from epilepsy, migraines, as well as other cerebrovascular or psychiatric disorders and also fevers and intoxication.While fever is commonly a source for the syndrome to arise in adults, children usually develop this condition in a different way – and that is encephalitis, specifically the type caused by the infection with the Epstein-Barr virus.Because the syndrome is only associated with underlaying causes and not a disease by its own, treatment varies from patient to patient, as it reflects the original developed condition. 2. Alien hand syndrome The alien hand syndrome stands out as one of the more unique entries onthis list, especially due to 2 important factors - the first one being the fact that this condition is manifested physically (in the limb), and the second being the mandatory past trauma for the disease to appear, rather than developing on a preexisting psychological disorder.While the effects of this condition may vary, symptoms mostly follow involuntary movement in one arm, often with no awareness or control. These movements include the limb grasping, lifting by itself, and even developing more complex patterns – such as undoing the action of the other hand – a phenomenon called intermanual conflict. In one peculiar case, a woman reported that her limb affected by Alien Hand syndrome tried to strangle her, however, this most likely not a reliable outcome to look after.What makes this syndrome hard to deal with outside the obvious suffering of the patients is also represented by the variety of possible causes for this condition. As we previously mentioned, Alien Hand syndrome appears after cerebral trauma – incidents like strokes, tumors, cerebral lesions and cerebral atrophy caused by neurodegenerative diseases are some examples of brain trauma that can (in very rare cases) lead to the condition.The most often cause, however, is a cerebral lesion, which is known to affect the right hemisphere and also the corpus callosum, that connects the two hemispheres. The frontal lobes are responsible with the voluntary and executive movements and actions, which means that damaging them can disrupt communication between the left and right hemispheres. This can result in one hand acting voluntarily, while the other one doesn’t.After studying the condition, some medical specialists are starting to considerate this syndrome as having 2 subtypes, each one with a different cause and effect:1) The first subtype is frontal, and is being caused by damage to the medial prefrontal cortex – this results in involuntary grasping and groping;2) The second subtype is callosal, which means the trauma is located at the corpus callosum – this is the subtype that is characterized by intermanual conflict.Recognizing the syndrome is also extremely important for the patient, as many other conditions can feel similar, although require completely different treatment. Similar diseases that share striking similarities can be:- movement disorders (such as Parkinson’s disease, chorea and also tics);- psychiatric disorders (including schizophrenia and depersonalization);- delusional disorders (in this case, the belief that one’s own limb is being controlled by someone else or not in their control).Treatment for Alien Hand syndrome can include both medication (such as botulinum toxin A and benzodiazepines), but also therapy – methods here vary from visuospatial coaching, cognitive-behavioral therapy (this reduces anxiety) and mirror box therapy (in which a mirror is placed between the hands, in order to trick the brain to view the reflected image as part of the body). 3. Capgras syndrome As the list goes on in depth and conditions become more and more obscure,a pattern that may become visible is the delusional factor between many of these following syndromes. In shorter terms, many of these diseases feature reality and sense distortion for the patients, which makes up for both the disturbing behavior of the ones affected and a difficult understanding on the condition by medical specialists. On of these syndromes is Capgras.Capgras is, like mentioned before, a delusion, in which one starts to strongly believe that a person they knew has been replaced with an identical imposter. While this is the main characteristic of the condition, other effects can be visible as well, including paranoia, aggressive behavior and also disorganized speech.As the theme of the list suggests, Capgras in extremely rare – as statistics indicate, only about 3% of the hospitalized psychosis patients also experience Capgras syndrome.While Capgras typically has higher chances of developing among people already affected by psychiatric conditions such as schizophrenia, schizoaffective disorder, and bipolar disorder, it can also arise in people that experienced cerebral trauma, similarly to the previously discussed Alien Hand syndrome. In this category we include people that suffered brain injuries, but also Alzheimer’s disease, different types of dementia and multiple sclerosis.Some researchers believe that Capgras is triggered by a disruption between the temporal lobe and limbic system – this damages the ability to recognize faces and associate them with emotions.Identifying Capgras among other conditions is crucial in order to determine a correct and effective treatment. Unfortunately, since so little is known about this condition, there is almost no research upon the effectiveness of different treating agents, although antipsychotic medication is usually effective at treating it. 4. Fregoli delusion Similarly to Capgras, Fregoli delusion also involves one’s strong beliefs regarding the false identity of someone, but with its unique twist. Unlike Capgras, that makes patients believe that an imposter replaced someone they knew, in Fregoli the situation is opposite – that a familiar person is disguising themselves as someone else, or even multiple people, in order to follow them.Fregoli is most common among those who already suffer from a psychotic disorder (which is most common schizophrenia), but also other conditions, such as a stroke, traumatic brain injury or a neurodegenerative disease. The cerebral lesions of Fregoli patients usually appear in the frontal lobe or on the right side of the brain.Treatment of the Fregoli delusion consists of antipsychotic medication (in the case of patients that developed the condition after a psychotic syndrome) and also cognitive-behavioral therapy. 5. Stendhal syndrome Stendhal syndrome features a very particular mental anomaly – and that is experiencing strong physical and emotional disturbances when viewing or interacting with art, or other beautiful, artistic elements.At first glance, the manifestation of this condition can feel bizarre and oddly specific, and quite frankly, the obscurity of the syndrome is also enhanced by the lack of diagnostic recognition. It is only thanks of the recent studies and medical reports that Stendhal became considered a distinct phenomenon. The symptoms vary extremely much, including episodes of increased heart rate, dizziness, fainting, epigastric pain, anxiety, euphoria and even exaltation. As you probably already figured out, the effects are mostly psychological and altogether relevant in the case of emotional distress. While concentrated forms of art such as galleries and museums are mostly known for causing this phenomenon, the beauty of nature is also recognized to being a triggering factor. Other possible triggers medical professionals suggested include repressed sexual drives, fatigue, sleep deprivation, the feeling of uncertainty or change in one’s life or even reaching the end of an important trip.For example, a well case of Standhal dates from 1817, when a French author experienced the condition after a trip to Florence, which resulted in the condition also being called Florence syndrome. Another name for the disease is hyperculturemia.A similar syndrome, called Jerusalem syndrome, also exists, in which the condition develops after the religious pilgrims finally reach their destination, the holy city. Medical experts actually explained that people who go on highly meaningful religious or personal trips as well as those with a history of mental illness share an increased risk to develop this syndrome, even though it is extremely rare as a whole.Scientists believe that the syndrome is caused by neurological processes that affect emotional processing, social situations and also introspection. In extreme cases of Stendhal, patients experience transient paranoid psychosis, disorientation, confusion and also strong anxiety that can lead to panic attacks – euphoria and exaltation are also possible symptoms, as mentioned previously. Treatment for the condition is determined after the patient’s history is available, in order to identify the highly variable syndrome correctly, among other disorders. Antipsychotics are used especially for patients that already have a psychotic disorder, although the episodes can also be resolved on their own. 6. Cotard delusion Continuing the list with one of the more disturbing entries, Cotard delusion brings in a phenomenon hard to comprehend at first – one’s feeling and strong belief that they have died. While syndromes range from rejecting one’s organs and feeling a sensation of decomposition to auditory and olfactory hallucinations, the most common way for people affected by the syndrome to express their condition is to simply state: “I am already dead.”Medically, this is known as a nihilistic delusion. The condition is also called Corpse Syndrome. Although most cases of Cotard are based on schizophrenia, the condition can also develop on other psychotic disorders, severe depression and bipolar disorders but also infections of the central nervous system, traumatic brain injuries, tumors or temporal lobe epilepsy – the last ones being possible physical damaging triggering factors, themed across some of the previously discussed syndromes as well, such as Capgras and Fregoli.The brain scans made on Cotard patients reveal that the condition may be caused by abnormalities in the frontal and temporal lobes – these are associated with functions such as self-awareness and the processing of reality. Treatment for Cotard is especially complex, with its blend of medication and therapy.Medication typically consists of antipsychotics – here we include olanzapine, clozapine, pramipexole and aripiprazole – these can be taken by themselves or complemented by antidepressants and mood stabilizers.Therapies that proved effectiveness are electroconvulsive therapy, but also behavioral and psychotherapies – however these have to be adapted depending on the patient. 7. Clinical Lycanthropy By “lycanthropy”, also known as shapeshifting, we understand the mythical power that allowed the man to transform into an animal, most commonly associated with a wolf or werewolf.As the name suggests, this condition makes the patient strongly believe that they can turn into an animal, any particular one. During episodes of hallucination, people affected are known to behave like animals and are sometimes even found hidden in forest areas or wild habitats.The condition itself is labeled as a type of delusional misidentification syndrome – this is strongly associated with psychotic disorders, but also depression or bipolar disorder.Because of this, treatment usually consists of antipsychotics, as it’s often effective, but antidepressants and mood stabilizers can also be administered, if other symptoms arise. 8. Depersonalization / Derealization disorder The conditions of depersonalization and derealization are heavily tied with the patient’s broken perspective on reality. People affected by this disorder often feel separated from their own bodies, even feeling that they are watching themselves. They can also believe elements around them and surroundings are not real and even the fact that time itself is distorted – either feeling slower or faster.Because the condition causes distress and anxiety over time, treatment includes a combination of medication and psychotherapy.However, it is highly important that the symptoms persist in order for the condition to be classified as the official syndrome. Doctors remind us that similar symptoms can also appear temporarily due to the effect of medication, drugs, and also other physical and mental health conditions. 9. Apotemnophilia This condition, also known as body integrity disorder, is a disturbing medical syndrome in which the one affected starts to feel an overwhelming desire to amputate healthy parts of their body.Despite the scary factor of the condition, little is actually known about it, although it is believed to be neurological, and may be linked to damage to the right parietal lobe.Treatment is difficult to be offered as many of the confirmed cases don’t seek medical attention, believing that amputating the desired part of the body is the right thing to do, leading to potential self-harm.However, when the patient is hospitalized, both cognitive behavioral therapy and aversion therapies are attempted in treating the condition. 10. Delusional parasitosis Also known as delusional infestation or the Ekbom syndrome, this severely disturbing condition features the unshakable belief of the affected person that their body is infested with bugs or other parasites.Syndromes are especially convincing for the patients – sensory hallucinations trigger extremely realistic sensations such as crawling, biting or stinging (which is medically called formication).Because the ones affected by the syndrome feel a desire to dig off whatever they think is crawling under their skin, physical wounds such as skin damage, ulcers and infections can also appear as a result of involuntarily self-harm. Although the syndrome can appear by itself, it can be also triggered by other conditions such as schizophrenia, dementia or depression. It can also develop from organic sources, including B12 deficiency, diabetes and drug use (especially cocaine and amphetamines). Treatment for the condition includes antipsychotic medication, as well as building a trusted relationship between the patient and specialists in order for the underlying psychological causes to be examined. In the end, we are left with the careful breakdown of these more than certainly overwhelming conditions. Some of them being more obscure and disturbing than the others on this list. However, at the end of the day, what we are left with are these peculiar cases, waiting to be understood, discovered and meticulously analyzed, for the love of the souls that fight them every single day, and for the love of the endless ocean of medical knowledge, some still waiting to be discovered by us… Sources: - https://www.clinicaladvisor.com/factsheets/rare-psychological-disorders-list/ - https://online.csp.edu/resources/article/10-rare-mental-health-conditions/ - https://en.wikipedia.org/wiki/Clinical_lycanthropy - https://my.clevelandclinic.org/health/diseases/9791-depersonalization-derealization-disorder - https://en.wikipedia.org/wiki/Delusional_parasitosis - https://pmc.ncbi.nlm.nih.gov/articles/PMC10871419/ - https://www.health.wa.gov.au/~/media/Files/Corporate/general-documents/Mosquitoes/PDF/160509_sn1a_DI-HiRes-final-for-the-web.pdf - https://www.healthline.com/health/mental-health/delusional-parasitosis
Every year on May 10, people around the world recognize World Lupus Day, a time dedicated to increasing awareness and understanding of a complex and often misunderstood disease: Lupus.Lupus is a chronic autoimmune condition, which means the body’s immune system mistakenly attacks its own healthy tissues. This can lead to inflammation and damage in different parts of the body, including the skin, joints, kidneys, heart, and brain. Because it affects people in different ways, lupus is often called “the disease of a thousand faces.”One of the challenges of lupus is that its symptoms can vary widely and may come and go. Common signs include extreme fatigue, joint pain, skin rashes (especially a butterfly-shaped rash across the cheeks and nose), and sensitivity to sunlight. These symptoms can sometimes mimic other illnesses, making lupus difficult to diagnose.Although anyone can develop lupus, it most commonly affects women, particularly between the ages of 15 and 45. While there is currently no cure, advances in treatment have made it possible for many people with lupus to manage their symptoms and live active lives. Treatment often includes medications to reduce inflammation and regulate the immune system, along with lifestyle adjustments such as stress management and proper rest.By sharing information and raising awareness, we can help ensure that lupus is better understood and that those affected receive the attention and care they deserve. On May 10, take a moment to learn, share, and support the fight against lupus.
Our most recent webinar marked an important milestone for our club, and we’re pleased to share that it was a truly rewarding experience for everyone involved! Bringing together high school students from different grades in a virtual setting allowed us to continue fostering learning, collaboration, and growth, values that remain at the heart of our club.The session itself was engaging and insightful, covering different cases that sparked thoughtful discussion and participation. What stood out most, however, was the quality of interaction throughout the event. Attendees asked insightful questions, shared perspectives, and contributed to a dynamic exchange of ideas that extended beyond the presentation itself.The feedback we received afterward has been overwhelmingly positive. Participants highlighted the clarity of the content, and the smooth organization of the webinar. Many also expressed appreciation for the opportunity to connect with peers in such an accessible format. This kind of response reinforces that we are moving in the right direction as a club!We are especially encouraged by how well this webinar format was received. It opens up new possibilities for reaching a wider audience, inviting diverse speakers, and continuing to deliver high-quality educational experiences without the limitations of physical location.Overall, we are very happy to have organized this webinar and grateful to everyone who contributed to its success; whether by attending or presenting. This positive experience motivates us to continue exploring similar initiatives in the future.Stay tuned for more events as we build on this momentum and keep advancing our shared mission in the medical field!!
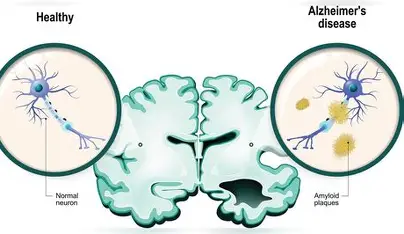
Alzheimer’s Disease – Everything You Need to KnowDisclaimer:As a student passionate about biomedicine, this article is a compilation of information from reputable sources. It is intended for educational purposes only.What is Alzheimer’s Disease?Alzheimer’s disease is one of the most serious and widespread neurological disorders in the world. It is a progressive brain disease that affects memory, thinking, and behavior, eventually interfering with a person’s ability to carry out daily activities. It is also the most common cause of dementia, accounting for the majority of cases globally.Alzheimer’s disease is a degenerative brain disorder that gradually destroys brain cells (neurons) and the connections between them. Over time, this leads to a significant loss of brain function and brain mass. The disease usually develops in older adults and progresses slowly over several years. It was first described in 1906 by neurologist Alois Alzheimer.Causes and Brain ChangesThe exact cause of Alzheimer’s disease is not fully understood, but it is believed to result from a combination of genetic, environmental, and lifestyle factors.At a biological level, Alzheimer’s is characterized by two abnormal structures in the brain:->Amyloid plaques – clumps of beta-amyloid protein that disrupt communication between brain cells->Neurofibrillary tangles – twisted fibers of tau protein that damage the internal structure of neuronsThese changes cause neurons to lose function, die, and eventually lead to brain shrinkage.SymptomsThe most common early symptom is memory loss, especially forgetting recent conversations or events.As the disease progresses, symptoms become more severe and include:Cognitive symptoms->Difficulty thinking, concentrating, and making decisions->Problems with language and finding the right words->Confusion about time and placeBehavioral and emotional symptoms->Mood swings and depression->Social withdrawal->Personality changes (anger, distrust, aggression)Functional difficulties->Trouble performing everyday tasks (cooking, dressing, managing money)->Getting lost in familiar placesIn advanced stages, patients may lose the ability to communicate, move, or care for themselves.Stages of Alzheimer’s DiseaseAlzheimer’s disease develops gradually in three main stages:1. Preclinical stage – brain changes begin before symptoms appear2. Mild cognitive impairment (MCI) – noticeable memory problems, but daily functioning is still possible3. Dementia stage – severe cognitive decline affecting daily lifeThe disease can last anywhere from 2 to 20 years, depending on the individual.Risk FactorsSeveral factors increase the likelihood of developing Alzheimer’s disease:->Age – the most important risk factor->Genetics and family history->Head injuries->Cardiovascular problems (high blood pressure, cholesterol, diabetes)->Poor lifestyle habits (lack of exercise, smoking, alcohol abuse)->Sleep disorders and social isolationAlthough age is the strongest risk factor, Alzheimer’s is not a normal part of aging.DiagnosisDiagnosing Alzheimer’s disease involves multiple steps:->Medical history and symptom evaluation->Memory and cognitive tests->Brain imaging (such as MRI or PET scans)->Biomarker tests (detecting amyloid and tau proteins)Modern diagnostic techniques allow doctors to detect the disease earlier than in the past.TreatmentThere is currently no cure for Alzheimer’s disease, but treatments can help manage symptoms and slow progression.Medications->Cholinesterase inhibitors (donepezil, rivastigmine, galantamine) – improve communication between brain cells->Memantine – regulates brain activity and may improve cognitionSupportive care->Managing depression, anxiety, and sleep problems->Providing structured routines and caregiver support->Prevention and LifestyleAlthough Alzheimer’s cannot be completely prevented, certain lifestyle changes may reduce the risk:->Regular physical exercise->Healthy diet (especially Mediterranean diet)->Mental stimulation and lifelong learning->Social engagement->Controlling cardiovascular risk factors (blood pressure, cholesterol, diabetes)ComplicationsIn advanced stages, Alzheimer’s can lead to serious health problems such as:->Infections (e.g., pneumonia)->Malnutrition and dehydration->Loss of mobility->Difficulty swallowingThese complications are often the cause of death in patients with Alzheimer’s disease.ConclusionAlzheimer’s disease is a complex and devastating condition that affects millions of people worldwide. It progressively damages memory, thinking, and independence, deeply impacting both patients and their families. While there is no cure yet, early diagnosis, proper treatment, and a healthy lifestyle can help slow its progression and improve quality of life.Understanding this disease is essential not only for those affected but also for society as a whole, as the number of cases continues to grow with the aging population.SourcesMayo Clinic. “Alzheimer’s Disease.” Mayo Clinic, 2025.https://www.mayoclinic.org/diseases-conditions/alzheimers-disease/symptoms-causes/syc-20350447Encyclopaedia Britannica. “Alzheimer Disease.” Britannica, 2025.https://www.britannica.com/science/Alzheimer-diseaseInstitutul Brain Map. “Boala Alzheimer – simptome, cauze și tratament.” Institutul Brain Map, 2025.https://institutulbrainmap.ro/boala-alzheimer-simptome-cauze-si-tratament/MedLife. “Alzheimer: cauze, simptome și tratament.” MedLife, 2025.https://www.medlife.ro/glosar-medical/afectiuni-medicale/alzheimer-cauze-simptome-tratament
Parkinson’s disease is a progressive neurological disorder that primarily affects movement, but its impact extends far beyond motor control. First described in 1817 by the British physician James Parkinson, the condition has since become one of the most studied neurodegenerative diseases in the world. Despite extensive research, it remains incurable, though treatments can significantly improve quality of life. Understanding Parkinson’s disease requires examining its causes, symptoms, progression, and the ongoing efforts to manage and eventually cure it.At its core, Parkinson’s disease is caused by the gradual degeneration of neurons in a specific area of the brain called the substantia nigra. These neurons are responsible for producing dopamine, a neurotransmitter that plays a crucial role in coordinating movement and emotional responses. As dopamine levels decline, the brain’s ability to regulate movement becomes impaired, leading to the hallmark symptoms of the disease.While the exact cause of neuronal degeneration is not fully understood, a combination of genetic and environmental factors is believed to contribute.The symptoms of Parkinson’s disease are typically divided into:- Motor symptoms include tremors, muscle rigidity, slowness of movement (bradykinesia), and impaired balance or posture. Tremors often begin in one hand or limb and may spread as the disease progresses. Muscle stiffness can make everyday tasks, such as walking or dressing, increasingly difficult. Over time, patients may develop a shuffling gait and experience frequent falls.- Non-motor symptoms can be equally, if not more, debilitating. These include depression, anxiety, sleep disturbances, cognitive decline, and autonomic dysfunction (such as problems with blood pressure regulation or digestion).The progression of Parkinson’s disease varies widely among individuals. In its early stages, symptoms may be mild and barely noticeable. As the disease advances, symptoms become more pronounced and can significantly interfere with daily life. In later stages, patients may require assistance with basic activities such as eating, bathing, and walking. Diagnosis of Parkinson’s disease is primarily clinical, meaning it is based on medical history and physical examination rather than a definitive laboratory test. Neurologists look for characteristic symptoms and may use imaging techniques to rule out other conditions. Early and accurate diagnosis is essential for effective management, although it can be challenging in the initial stages.Treatment for Parkinson’s disease focuses on managing symptoms, as there is currently no cure. The most commonly used medication is levodopa, which is converted into dopamine in the brain and helps alleviate motor symptoms. Other medications, such as dopamine agonists, are also used to enhance dopamine function. While these treatments can be highly effective, their benefits may diminish over time, and long-term use can lead to side effects such as involuntary movements. In addition to medication, non-pharmacological approaches play a vital role in managing the disease. Physical therapy can help maintain mobility and balance, while occupational therapy assists patients in adapting to daily challenges. Speech therapy may be necessary for those experiencing difficulties with communication or swallowing. Regular exercise has been shown to improve both motor and non-motor symptoms, highlighting the importance of an active lifestyle.Research into Parkinson’s disease is ongoing and multifaceted. Scientists are exploring the underlying mechanisms of neuronal degeneration, including the role of protein misfolding and inflammation. Advances in genetics have identified several genes associated with an increased risk of developing the disease. Additionally, researchers are investigating potential disease-modifying therapies that could slow or halt progression, rather than simply treating symptoms.One promising area of research involves stem cell therapy, which aims to replace damaged neurons with healthy ones. Another focuses on developing drugs that target alpha-synuclein, a protein that accumulates abnormally in the brains of individuals with Parkinson’s disease. While these approaches are still largely experimental, they offer hope for more effective treatments in the future.Living with Parkinson’s disease presents significant physical, emotional, and social challenges. Patients often require strong support systems, including family, caregivers, and healthcare professionals. Education and awareness are essential for reducing stigma and ensuring that individuals receive appropriate care and understanding.Parkinson’s disease is a complex and multifaceted condition that affects millions of people worldwide. Although it is primarily known for its impact on movement, its effects are far-reaching and deeply influence quality of life. While current treatments can manage symptoms effectively, the search for a cure continues. Ongoing research and advances in medical science provide hope that one day, Parkinson’s disease may be not only treatable but preventable or even curable.
“Disease is very old, and nothing about it has changed. It is we who change as we learn to recognize what was formerly imperceptible.” - Jean-Martin Charcot In 1868, a mysterious neurological condition finally received a name. The French neurologist Jean-Martin Charcot described and classified a disease he called la sclérose en plaques. Often regarded as the “Father of Neurology”, Charcot was the first to recognize this disorder as a distinct medical entity. The condition would later become known in English medical literature as Multiple Sclerosis (MS) [1]. Yet the story of MS did not begin with Charcot. Descriptions resembling the disease appear in medical writings dating as far back as the Middle Ages. What had been missing, however, was the scientific framework needed to connect symptoms observed in living patients with structural changes in the nervous system. The nineteenth century brought exactly that shift: physicians began pairing clinical observation with pathological anatomy. This methodological breakthrough allowed Charcot to link patients’ neurological symptoms with distinctive lesions - scattered sclerotic plaques - found in the brain and spinal cord during post-mortem examination [2][3]. From these observations emerged what is now known as Charcot’s triad, a set of hallmark symptoms that helped physicians recognize the disease. These include nystagmus, involuntary rhythmic eye movements; intention tremor, which appears during voluntary motion; and scanning speech, a distinctive form of dysarthria in which words are pronounced slowly and broken into syllables. Modern neuroscience has greatly expanded upon Charcot’s early insights. Today, multiple sclerosis is understood as a chronic autoimmune, neuroinflammatory, and neurodegenerative disorder affecting the central nervous system (CNS) [4]. Although decades of research have significantly advanced our knowledge, the precise causes of MS remain complex and not fully understood. What is clear, however, is the central role of demyelination - the destruction of the myelin sheath, the insulating layer that surrounds nerve fibers in the white matter of the brain and spinal cord [5]. Because myelin enables rapid and efficient electrical signaling between neurons [6], its degradation disrupts communication within the nervous system and can lead to a wide range of neurological symptoms, including impaired motor control. Historically, identifying MS was far from straightforward. The disease’s polymorphic presentation often led physicians to confuse it with other neurological conditions, particularly Parkinson’s disease, which had been described decades earlier under the name paralysis agitans. Both disorders could involve tremors and motor disturbances, making differentiation difficult. One of Charcot’s earliest and most influential cases involved his female servant, Luc, who had initially been diagnosed with shaking palsy. Through careful observation, Charcot noticed something unusual about her symptoms. Unlike Parkinsonian tremors, which occur continuously, Luc’s tremors appeared primarily during intentional movements. This subtle difference raised an important question: was this truly the same disease? The answer emerged after Luc’s death. During the post-mortem examination of her brain and spinal cord, Charcot identified distinctive sclerotic plaques distributed throughout the central nervous system. These lesions confirmed that the disorder he was observing was not Parkinson’s disease, but a separate and previously unrecognized neurological pathology [3]. Much of this pioneering work took place at the Hôpital de la Salpêtrière in Paris, where Charcot worked alongside his colleague Alfred Vulpian. Together, they helped define multiple sclerosis as a distinct clinical entity. Their early observations highlighted the severe prognosis associated with the disease and the widespread lesions found throughout the nervous system - features that remain central to MS diagnosis today. They also recognized something that continues to challenge neurologists even now: MS rarely presents the same way twice. Because lesions can appear in different regions of the central nervous system - spinal, cerebral, or both - the symptoms can vary widely between patients. This variability is one of the defining characteristics of multiple sclerosis and remains a key challenge in both diagnosis and treatment. These early discoveries laid the foundation for more than a century of neurological research. From Charcot’s first observations of mysterious plaques in the nervous system to today’s advanced imaging techniques and molecular studies, our understanding of multiple sclerosis has evolved tremendously. Yet many questions remain unanswered. Despite significant therapeutic progress, MS continues to be an incurable and highly complex disease. Understanding its mechanisms - from immune dysregulation to demyelination and neurodegeneration - remains one of the central challenges of modern neuroscience, and a crucial step toward developing treatments that can not only slow the disease but ultimately repair the damage it causes. Bibliography: 1. B. Zalc. One hundred and fifty years ago Charcot reported multiple sclerosis as a new neurological disease. Brain. Vol. 141, Issue 12, pg. 3482-3488, 2018, https://pmc.ncbi.nlm.nih.gov/articles/PMC6262215/. 2. Harvard Medical School Library - Countway Library of Medicine. Medical treatment in the nineteenth-century. Apothecary Jars Exhibit. https://collections.countway.harvard.edu/onview/exhibits/show/apothecary-jars/nineteenth-century-treatment. 3. Z. G. Reyes. Sclérose en Plaques: A Tribute to the History of Multiple Sclerosis and Charcot’s Role in Precision Medicine Today. American Academy of Neurology Medical Student Essay Award. 2023, https://www.aan.com/siteassets/home-page/education-and-research/research/award-winners/scientific-award-winners/2023-winners/reyes_zabrina_medical_student_essay.pdf. 4. A. H. Maghzi, A. Borazanci, J. McGee, J. S. Alexander, E. Gonzalez-Toledo, A. Minagar. 1 - Multiple Sclerosis: Pathophysiology, Clinical Features, Diagnosis, and Management. Neuroinflammation. pg. 1-23, 2011, https://www.sciencedirect.com/science/chapter/edited-volume/abs/pii/B9780123849137000010?via%3Dihub. 5. J. M. Greer, P. A. McCombe. Role of gender in multiple sclerosis: Clinical effects and potential molecular mechanisms. Journal of Neuroimmunology, vol. 234, issues 1-2, pg. 7-18, 2011, https://www.sciencedirect.com/science/article/abs/pii/S0165572811000658. 6. P. Morell, W. T. Norton. Myelin. Scientific American, vol. 242, no.5 (May 1980), pg. 88-119, https://www.jstor.org/stable/24966326.

What Is Sunscreen? Sunscreen is a product applied to the skin to safeguard it from the sun’s harmful rays. It works by blocking or reducing ultraviolet (UV) radiation so that it does not damage the skin. The sun emits UV radiation, an invisible type of light that can be harmful. Two types are particularly important: UVB and UVA rays. UVB rays cause sunburn and contribute to skin cancer, while UVA rays affect deeper skin layers, leading to skin aging, such as wrinkles and dark spots, and also contribute to skin diseases. Most sunscreen products display an SPF number, which indicates how well they protect the skin against UVB rays. Although no sunscreen can block all UV radiation, proper use provides significant protection and helps prevent sunburn and skin damage. Why Is Sunscreen Important? Sunscreen helps prevent sunburn and preserve the integrity of the skin. In addition, it reduces the risk of skin cancer and slows down premature skin aging, making it an essential part of daily skin care. Strategies to Reduce Sun Damage To diminish sun-related skin damage, it is recommended to use a broad-spectrum sunscreen with an SPF of at least 30, applied 15–30 minutes before sun exposure. It is essential to reapply every two hours and ensure that all exposed areas, including the face, ears, neck, hairline, and arms, are covered. Combining sunscreen with protective clothing, hats, and seeking shade further enhances skin protection.

Many important medical discoveries were made thanks to chance, curiosity, and careful observation. In some cases, scientists did not get the results they expected, but instead of ignoring them, they chose to investigate further. These moments changed the course of medicine. One of the most famous examples is penicillin. In 1928, Alexander Fleming noticed that a mold called Penicillium had grown in one of his Petri dishes and killed the bacteria around it. Although this happened by accident, Fleming understood its importance. This discovery later led to the development of antibiotics, which have saved millions of lives by treating bacterial infections. Another important discovery is related to anticoagulants. Chemist Karl Paul Link began studying cases in which cattle were bleeding without an obvious reason after eating moldy clover. His research helped identify substances that prevent blood from clotting. Even though these substances were first used as rat poison, they were later adapted for medical use and are now essential in treating heart diseases and preventing strokes. Some medical inventions were also the result of technical mistakes. The pacemaker is a good example. While early versions were created by Rune Elmqvist and Åke Senning, Wilson Greatbatch later improved the device after accidentally building an incorrect electrical circuit. He realized that the device could control heartbeats. In 1960, the first pacemaker was successfully implanted in a human patient, helping people with heart rhythm problems live longer lives. Another major breakthrough in medicine was anesthesia. In the 19th century, Horace Wells observed that substances such as nitrous oxide and ether could reduce pain. Although his early attempts at painless dental procedures were not successful, the idea continued to develop. William Morton later proved that anesthesia worked, making modern surgery possible and greatly reducing pain during medical procedures. These examples show that progress in medicine does not always come from perfect planning, but often from curiosity and the ability to learn from unexpected situations.